The most lethal and common subtype of ovarian cancer starts in a tissue we cannot biopsy non-surgically: the fallopian tube.
We are building a device to collect cells directly from the fallopian tube and analyse them like a biopsy. The result is a non-surgical answer as to whether women are in the early stages of developing ovarian cancer — allowing informed, early intervention, before they have to give up their ovaries.
of all ovarian cancer is high-grade serous: the lethal subtype that starts in the fallopian tubes
5-year survival rate for the 80%+ women diagnosed with ovarian cancer at stage 2 or later
of risk-reducing ovary and tube removals show no cancer or precursor lesions at surgery
Ovarian cancer is often found too late, due to its vague symptoms and the lack of effective screening and early diagnosis methods.
Its deadliest subtype, high-grade serous, originates in the fallopian tube.
However, the tissue cannot be assessed without surgery; it must be removed for analysis for early cancerous signs.
For high-risk women, the choice is therefore prevention through surgery or waiting for disease to emerge.
References
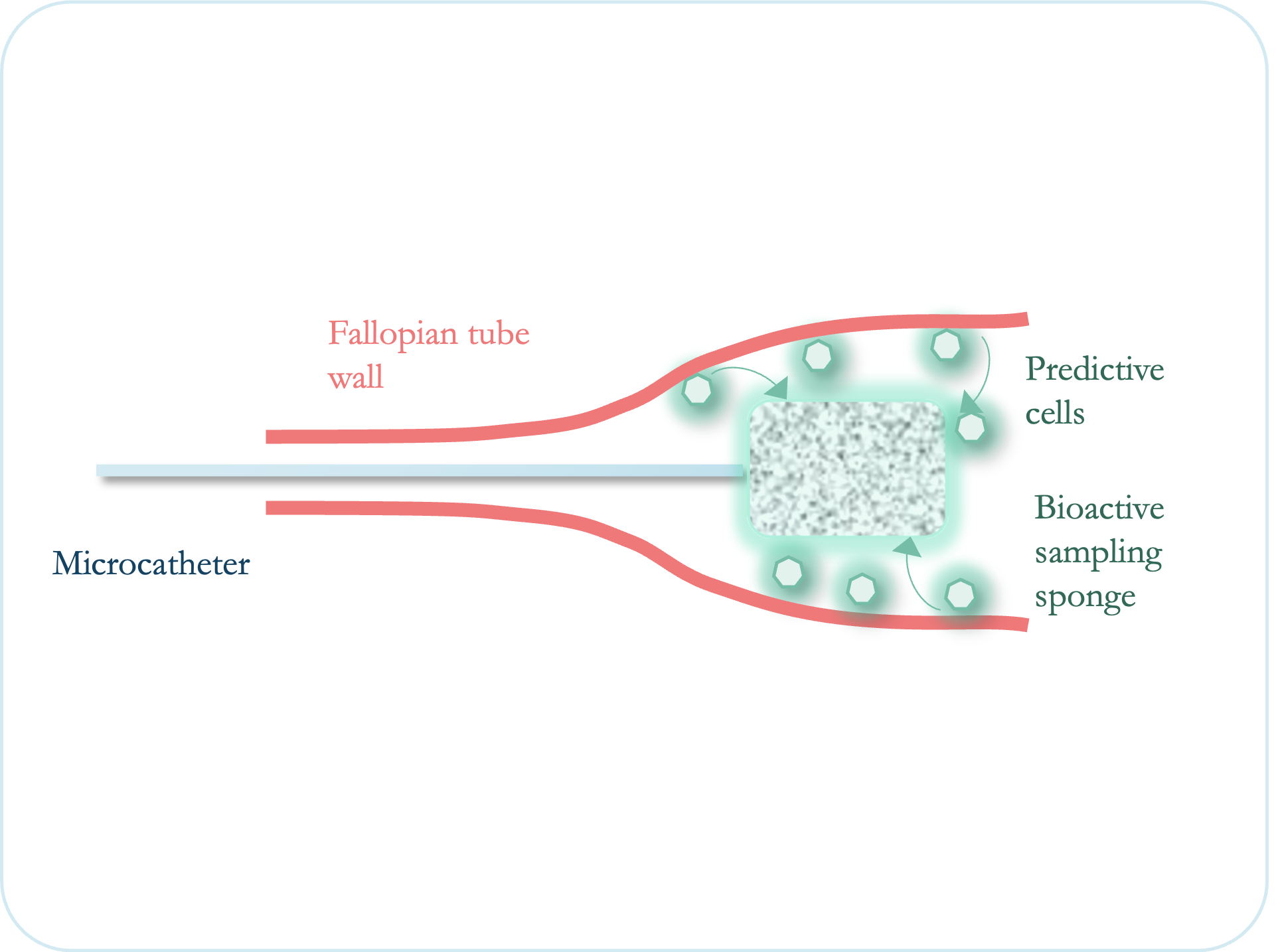
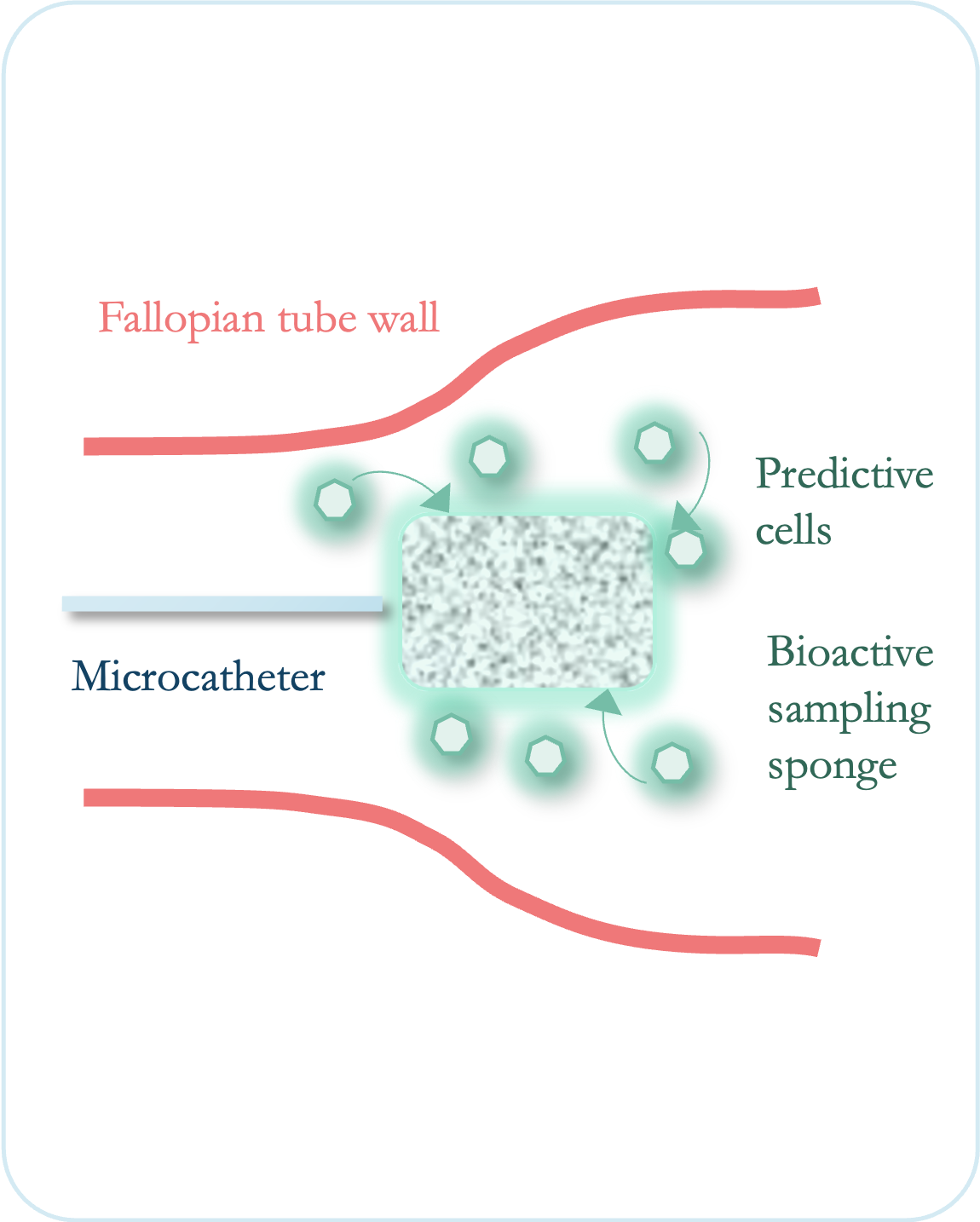
To address the clinical problem, we are developing a medical device designed to access and sample the full length of the fallopian tubes using a hysteroscopic microcatheter-based approach.
At its tip, our patented biomaterial technology is intended to capture disease-relevant precursor cells and enrich material for standard histological analysis.
By enabling access to biologically relevant material earlier in the disease pathway, the platform is intended to support earlier and more informed intervention — shifting the paradigm from prophylactic surgery to early, therapeutic intervention, preventing cancer as early as possible.
Patient's fallopian tubes are sampled with the microcatheter. Procedure is conducted under no / local anaesthetic in an office-based / outpatient setting.
Microcatheter tips are analysed by histopathology for presence of cancerous cells, like a biopsy sample.
Based on the pathology result, a decision is taken to proceed with risk-reducing surgery or defer.
Many diseases are detected too late because existing tests do not consistently capture high-quality biological material from the right anatomical locations — especially in early or asymptomatic disease.
Advances in circulatory biomarkers and molecular diagnostics have outpaced our ability to collect representative local samples, particularly from hard-to-access sites typically only accessed through local biopsy and subsequent pathology-based analysis.
Xeparate is therefore built around a simple premise: sample relevant biomarkers from disease sites without the need for a biopsy, or where biopsies are not possible.
Xeparate is developing a proprietary medical device platform for local biological sampling before biopsy.
Our technology is being developed for clinical and screening settings where current sampling methods fall short or do not yet exist.
The platform is intended to be adaptable across multiple indications over time, with an initial focus on oncology. Our design approach is centred on fitting into existing clinical workflows while improving the quality of the material collected.
Three pillars
Accessing disease-relevant biological material.
Adapts to existing catheter and endoscope-based procedures.
Integrates with existing downstream pathology-based analysis.
Built to support

Biomaterials advisor

Clinical advisor

Biochemistry advisor
